





Spinal fractures and deformities; It is a condition in which the vertebral bones that make up the spinal column lose their structural integrity due to trauma, disease or old age and the normal anatomical curvature of the spine is disrupted.
These conditions not only affect the bone structure but can also lead to severe neurological losses by suppressing the spinal cord and nerve roots passing through the spinal canal.
What is a Spinal Fracture?
A spinal fracture is the disruption of the integrity of one or more of the 33 vertebrae extending from the neck area to the coccyx.
Spine; It is the main carrier column of the body and protects the central nervous system.
When a fracture occurs, the load-bearing capacity of the spine decreases and the displacement of fracture fragments towards the spinal cord leads to an unstable picture we call “instability”.
In modern medicine, these fractures; It is evaluated by looking at how much of the bone is damaged and whether the nerve tissue is in danger.
What are the Symptoms of Spinal Fracture?
The clinical picture of a spinal fracture varies widely depending on the severity of the fracture and whether there is nerve compression.
- Sudden and Severe Back/Low Back Pain: Sharp pain that usually starts at the time of trauma and increases with movement, coughing or deep breathing.
- Limitation of Movement: Loss of flexibility of the spine and the patient’s inability to bend forward or rotate.
- Neurological Losses: Sudden onset of numbness, tingling, pins and needles sensation or complete loss of strength (paralysis) in the arms or legs.
- Muscle Spasms: Involuntary stiffening of the muscles in the fracture area to protect the spine.
- Shortening of Stature and Deformity: Noticing a shortening in height as a result of bending the spine forward (hunchback), especially in osteoporotic compression fractures.
- Loss of Bladder and Bowel Control: It is a critical symptom that indicates advanced spinal cord compression and requires immediate surgical intervention.
According to Assoc. Prof. Dr. Erdinç Özek; “Pain in a spinal fracture is the most important alarm signal given by the body. However, not every fracture manifests itself in paralysis. Especially in elderly patients with osteoporosis, back pain that starts after a simple sneeze or slight bending may be a sign of a ‘silent compression fracture’. At this point, it is vital not to pass off the pain by just saying ‘old age pain’.”
Causes of Spinal Fracture
Spinal fractures usually occur when a high-energy force exceeds bone resistance or when the resistance of the bone decreases due to diseases.
- High-Energy Traumas: Traffic accidents, falls from heights (work accidents, balcony falls) and firearm injuries.
- Osteoporosis (Bone Resorption): As a result of decreased bone density, especially in postmenopausal women and older men, the spine collapses by not even being able to carry its own weight.
- Pathological Causes: Cancer metastases or bone marrow diseases (such as Multiple Myeloma) that spread to the spine weaken the bone to the size of an “eggshell”, making it vulnerable to fracture.
- Sports Injuries: Neck fractures caused by diving into shallow water or sudden twisting movements that occur in contact sports.
Clinical Experience Note (Anonymous Case): A 68-year-old female patient presented with a sudden onset of back pain after lifting a heavy object while cleaning at home. In the detailed imaging of the patient, who was followed up only with the suspicion of “herniated disc” in the other center, a fresh compression fracture was detected at a rate of 40% in the T12 (back-waist junction) vertebra due to osteoporosis. After the 20-minute ‘Kyphoplasty’ (balloon bone lift) procedure performed under local anesthesia, the patient’s pain decreased by 90% on the procedure table and he was discharged on foot on the same day.
Types of Spinal Fractures
Spinal fractures are classified according to the direction of the force and the way the bone is broken down. This classification is the most basic guideline we use when deciding whether the treatment will be surgical or not.
Compression Fractures (Compression Fractures)
It is usually the loss of height of the anterior part of the vertebral body due to pressure. The spine takes the shape of a wedge. It is mostly seen in the elderly with osteoporosis (bone loss) or mild falls. They usually do not cause nerve damage, but if left untreated, they can lead to permanent hunchback.
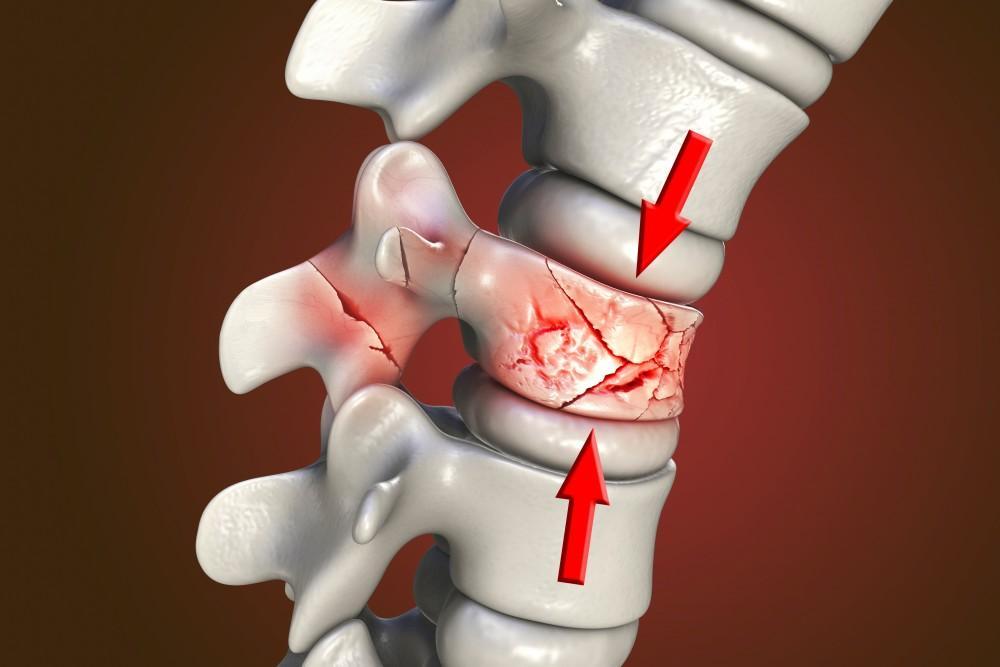
Burst Fractures (Burst Fractures)
It occurs with higher energy traumas (such as falling from a height on your feet). The vertebral body is broken down from both the anterior and posterior parts. In this type of fracture, the risk of displacement of bone fragments towards the back, that is, towards the spinal canal, is very high. This situation brings with it the risk of sudden paralysis.
Fracture Dislocations (Fracture Dislocations)
It is the most severe picture in which the spine is both broken and the alignment of the vertebrae on each other is disrupted, that is, it shifts. It is commonly seen in traffic accidents or severe rotational impacts where seat belts are not fastened. The risk of spinal cord injury is highest in this group.
What are Spinal Deformities?
Deformities are the deterioration of the three-dimensional alignment of the spine. These are sometimes congenital, and sometimes they occur as a result of malunion of spinal fractures in old age.
Scoliosis
It is a lateral curvature of the spine to the right or left of more than 10 degrees. It involves not only a simple curvature, but also the rotation of the vertebrae around their axis (rotation). While it can be managed with a brace when diagnosed early, advanced degrees require surgical correction.
Kyphosis (Hunchback)
It is the excessive increase in the convex curvature that normally exists in the back region of the spine. The vertebrae, which become “wedged” after age-related osteoporotic fractures, cause the patient’s torso to collapse forward. This condition is not just an aesthetic problem; It is also a pathology that reduces lung capacity and causes severe back pain.
Diagnostic Methods
The correct treatment is to clarify the type of fracture and the “instability” (imbalance).
- Direct X-ray (X-ray): It is the first evaluation to see the general alignment of the spine and major fractures.
- Computed Tomography (CT): It shows the architecture of the bone down to the smallest detail. It is the “gold standard” for understanding how far fracture fragments have entered the spinal canal.
- Magnetic Resonance (MRI): It is indispensable to see edema in the bone (whether the fracture is new or old), damage to the spinal cord, the condition of the ligaments and discs.
- Bone Densitometry: It is used to determine whether there is an underlying bone resorption (osteoporosis) of the fracture.
Assoc. Prof. Dr. Erdinç Özek said, “The most critical distinction we make during the diagnosis phase is whether the fracture is ‘stable’ (safe) or ‘instable’ (mobile). While stable fractures can heal with a corset; Unstable fractures require surgical stabilization (screwing) as they increase the risk of nerve damage with every movement of the patient. Making a decision only with x-rays without taking an MRI means overlooking a hidden spinal cord injury.”
| Fracture Type | Risk of Nerve Damage | Treatment Approach |
| Compression Fracture | Low | Corset or Kyphoplasty (Closed) |
| Burst Fracture | Medium / High | Stabilization Surgery |
| Fracture Dislocation | Very High | Emergency Surgery and Instrumentation |
Clinical Experience Note (Anonymous Case):
In a young patient who applied to the patient standing after a traffic accident saying “my back hurts”, the condition, which at first glance seemed like a simple pain, was diagnosed as an “unstable burst fracture” by CT and MRI examination. The patient was immediately hospitalized and stabilized by microsurgical method; Thus, a possible paralysis that may develop when the patient stands up is prevented.
Spinal Fracture Treatment Methods
Treatment strategy in spinal fractures; The stability of the fracture is determined by the patient’s age, bone quality and risk of neurological damage.
Our main goal is to stabilize the spine, relieve pain and return the patient to his active life as soon as possible.
Conservative Treatment (Corset and Rest)
It is preferred in stable compression fractures that do not carry the risk of nerve damage and where more than 50% of the spinal height is preserved.
Body corsets (TLSO corsets) specially prepared for the patient reduce the load on the fracture area and allow the bone to fuse naturally. Close follow-up in this process is critical to prevent the fracture from turning into a “humpback” (progressive kyphosis).
Closed Spine Surgeries (Kyphoplasty and Vertebroplasty)
They are “minimally invasive”, that is, closed methods, which are generally applied in compression fractures due to osteoporosis or tumors.
- Vertebroplasty: Medical bone cement (polymethylmethacrylate) is injected into the fractured vertebra with a special needle.
- Kyphoplasty: A balloon is first placed inside the collapsed bone and inflated to restore bone height, and then the resulting cavity is filled with cement.
- Advantage: It can be performed under local anesthesia, does not require stitches and the patient can stand up on the same day.
Surgical Treatment (Instrumentation and Fusion)
It is the procedure performed to stabilize the spine in comminuted blowout fractures or fractured dislocations.
In this method, popularly known as “platinum insertion”, titanium screws (pedicle screws) and rods are placed in the intact vertebrae above and below the fractured vertebra. If there is spinal cord compression, the nerves are relieved by opening the bone windows (laminectomy) during surgery.
According to Assoc. Prof. Dr. Erdinç Özek; “Our philosophy in modern spine surgery is ‘intervention as needed’. If we can treat a fracture with the closed method (Kyphoplasty), we do not put the patient under great surgical stress. However, if there is bone compression on the spinal canal, it is inevitable to remove this pressure with microsurgery and to establish a solid structure with instrumentation.”
| Treatment Method | Application Time | Hospital Stay | Speed of Recovery |
| Corset Treatment | 6 – 12 Weeks | No Need / 1 Day | Slow |
| Kyphoplasty (Closed) | 30 Minutes | 1 Day | Very Fast (Instant) |
| Surgery (Screwing) | 2 – 4 Hours | 3 – 5 Days | Medium (with rehabilitation) |
Recovery Process After Spine Surgery
The postoperative process differs according to the technique of the method applied.
- First Move: In closed surgeries, the patient is walked 2 hours later, and in open surgeries, the next day, usually accompanied by a physiotherapist.
- Wound Care: While wound care is not required in minimally invasive procedures, stitches are removed on the 15th day in open surgeries.
- Restrictions: For the first 2-3 months, it is forbidden to lean forward, carry heavy loads and make sudden twisting movements.
- Physical Therapy: Early rehabilitation in patients with muscle weakness after surgery accelerates nerve healing.
Frequently Asked Questions
Can every pain in my back be a sign of fracture?
No, but especially in the elderly, even if there is no trauma, sudden onset of back pain that makes breathing difficult should be checked with imaging (CT/MRI).
Do spinal screws (sinkers) stay in the body for life?
Yes, they are usually not removed unless they cause a problem. Modern titanium alloys are MR compatible and do not chirp in airport detectors.
Is there a risk of paralysis after surgery?
Thanks to advanced neuromonitoring technologies, the condition of the nerves is monitored instantly during surgery. This technology has increased surgical safety to over 99%.
Resource and Expert Knowledge
This information has been arranged with reference to Assoc. Prof. Dr. Erdinç Özek’s advanced spinal surgery techniques and deep expertise in trauma surgery and the medical literature of 2026. Assoc. Prof. Dr. Erdinç Özek is a surgeon with a high success rate in the correction of complex spinal deformities and closed bone strengthening surgeries.
