




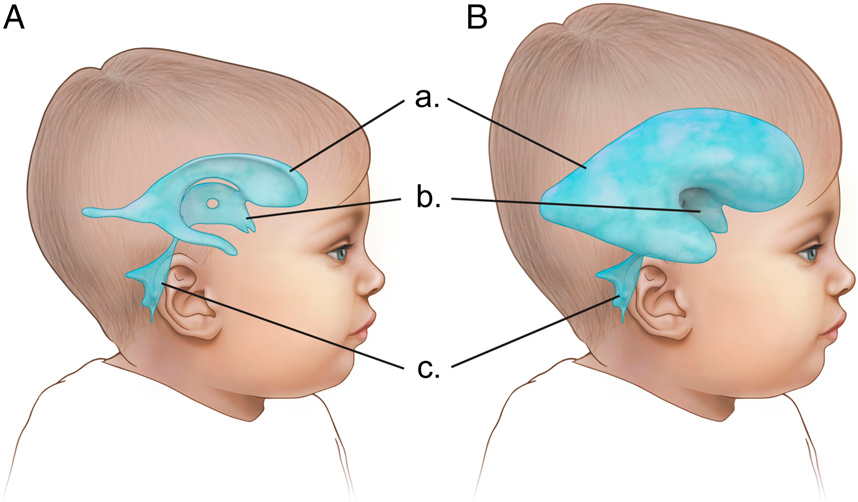
Childhood hydrocephalus; It is a condition in which cerebrospinal fluid (CSF) accumulates in the head due to an imbalance in the production, circulation or absorption pathways, resulting in enlargement of the brain ventricles and an increase in intracranial pressure.
This condition, popularly known as “fluid collection in the brain”, is a disease that can cause irreversible damage to the developing brain tissue if not intervened in the early period, but can be successfully managed with modern neurosurgical methods.
What is Childhood Hydrocephalus?
Hydrocephalus is a disruption of the dynamics of cerebrospinal fluid, the vital fluid of the central nervous system.
Under normal conditions, this fluid protects the brain from external impacts, transports nutrients and cleans waste products.
If there is an obstacle (tumor, cyst, adhesion) in the flow path of fluid or blockage of the absorption ducts, the cavities inside the brain (ventricles) begin to expand like a balloon filled with water.
In childhood, this condition causes abnormal growth around the head because the skull bones have not yet fully fused; After the bones fuse, it directly compresses the brain tissue, leading to loss of function.
Symptoms and Signs of Hydrocephalus in Children
The clinical picture of hydrocephalus is examined in two main groups according to the age of the child and the closure of the skull bones (sutures).
Symptoms of Hydrocephalus in Infants
Since the skull is flexible during infancy, symptoms are usually manifested by physical changes:
- Abnormal Head Growth: Head circumference far above the percentile curves.
- Fontanel Tension: The soft area on the top of the head is bulging and hard outwards.
- “The Setting Sun” View: Downward shifting of the eyeballs and prominence of the upper part of the whites of the eyes.
- Nutritional Disorder: Reluctance to suck and gushing vomiting.
- Extreme Restlessness or Sleepiness: The baby is much more tearful than usual or too weak to wake up.
Symptoms of Hydrocephalus in Children and Adolescents
In older children, the head cannot expand because the skull bones are closed; This causes intracranial pressure to rise rapidly:
- Severe Headache: Pain that is more pronounced especially in the morning and relieves after vomiting.
- Visual Disturbances: Double vision, blurred vision, or crossed eyes.
- Decline in School Success: Impaired concentration, memory problems and learning difficulties.
- Balance and Gait Problems: Frequent falls, loss of coordination in walking.
- Personality Changes: Irritability or decreased interest in the environment.
According to Assoc. Prof. Dr. Erdinç Özek; “The biggest helper of families is follow-up charts. A disproportionate increase of 1-2 centimeters in head circumference in babies can sometimes be a precursor to damage that will last for months. In older children, instead of thinking that ‘morning pains’ and ‘sudden changes in school performance’ are psychological, it is life-saving to undergo a neurological evaluation. In hydrocephalus, time means nerve cells.”
Comparison Table of Age-Specific Symptoms
| Symptom Type | Infancy (0-2 Years) | Childhood/Adolescence (Ages 2-18) |
| Physical Change | Rapid growth around the head | No physical growth |
| Eye Finding | View of the setting sun | Double vision (Diplopia) |
| Type of Vomiting | Gushing, post-feeding | In the morning, it squirts on an empty stomach |
| Cognitive Impact | Retardation in motor development | Decline in academic achievement |
Causes of Childhood Hydrocephalus
The development of hydrocephalus in children spans a wide spectrum, starting from the prenatal process to various factors in childhood.
It is possible to examine these reasons in two categories:
- Congenital Causes: These are anomalies that develop while the baby is still in the womb. The most common are conditions such as narrow fluid channels in the brain (Aquaduct Stenosis) or spinal openings such as Spina Bifida.
- Acquired Causes: These are conditions that occur after birth. Brain hemorrhages, infections such as meningitis, head trauma or brain tumors in premature babies can disrupt the flow of fluid and lead to hydrocephalus.
Hydrocephalus Diagnostic Methods
The imaging techniques offered by modern medicine clearly reveal not only the presence of hydrocephalus, but also where the fluid is stuck.
- Transfontanel Ultrasonography: It is a rapid screening method that is used in babies with the fontanel open, does not contain radiation and can be done at the bedside.
- Magnetic Resonance Imaging (MRI): It is the gold standard that shows the anatomical structure of the brain down to the smallest detail. The surgical decision is clarified with “Cine-MR” techniques that measure the flow rate of the fluid.
- Computed Tomography (CT): It is used in emergency situations to see ventricular enlargement within seconds in cases where intracranial pressure increases rapidly.
- Fetal MRI: It is applied to evaluate the brain development and fluid accumulation of the baby in the womb before birth.
Hydrocephalus Treatment Methods
The main goal of hydrocephalus treatment is to eliminate pressure on the brain and prevent permanent damage.
In this case, which cannot be treated with medication, two basic surgical options come to the fore.
Shunt Applications (Ventriculoperitoneal Shunt)
It is the most widely used method worldwide. It is a drainage system that transfers excess fluid from the brain to another part of the body (usually the abdominal cavity).
- How the System Works: A shunt consists of a thin catheter inserted into the brain, a one-way valve that regulates the flow of fluid, and a tube that carries fluid to the abdomen.
- Programmable Valves: Modern shunts used today are “programmable” in which the pressure setting can be changed with the help of an external magnet after surgery. This reduces the risk of the patient being operated on again.
Endoscopic Third Ventriculostomy (ETV)
It is a revolutionary “closed” method that eliminates shunt dependence in eligible patients.
- Application: A millimeter camera (endoscope) is entered into the brain and a new channel is opened at the base of the brain by bypassing the area where the blockage is located.
- Advantage: An external artificial device (shunt) is not inserted into the body. In this way, long-term risks such as shunt infection or shunt rupture are eliminated.
Assoc. Prof. Dr. Erdinç Özek; “Not every hydrocephalus patient is doomed to shunting. Especially in occlusive hydrocephalus, it is our priority to restore the natural fluid flow by endoscopic method (ETV). However, in cases where a shunt needs to be inserted, we aim to keep the patient’s comfort of life at the highest level by choosing ‘smart valve’ technologies. Do not forget that the millimetric pressure adjustments made after surgery are the key to success as well as the treatment method.”
Treatment Comparison Table: Shunt vs ETV
| Feature | Shunt Application | Endoscopic Method (ETV) |
| Method | An artificial drainage system is placed | A new channel opens in the brain |
| Foreign Body | Available (Shunt system) | None |
| Risk of Infection | Higher | Lower |
| Long-Term Follow-Up | Shunt revision may be required | Shutdown risk monitoring is required |
| Applicability | In almost all types of hydrocephalus | In certain types of (obstructive) hydrocephalus |
Shunt Surgery Process and Preparation
Shunt surgery is a standard but highly precise surgical procedure for treating hydrocephalus.
Before the surgery, the general health status of the child is evaluated in detail by the anesthesiologist and neurosurgeon.
- Preparation Phase: The child’s skin is cleaned with special solutions to minimize the risk of infection. If necessary, preventive antibiotic treatment is started before surgery.
- Application: It is performed under general anesthesia, a procedure that takes approximately 45-60 minutes.
- Technical Detail: The catheter, which is inserted into the brain through a small hole opened in the skull, is delivered to the abdominal cavity (peritoneum) through a tunnel passed under the skin.
Recovery and Follow-up After Shunt Surgery
The postoperative period is a critical phase in which the shunt is monitored to balance the intracranial pressure.
- Hospital Stay: Generally, an observation period of 24-48 hours is sufficient.
- Initial Checks: Immediately after surgery, the position of the shunt and ventricle sizes are checked with brain tomography or ultrasound.
- Pressure Adjustment: If a programmable (adjustable) valve is inserted, your doctor optimizes the valve pressure with an external device according to the child’s clinical response.
What is Shunt Revision?
Shunt revision is the process of surgically replacing part or all of the existing shunt system.
As children grow, the length of the installed pipes may be short or the system may lose its function due to calcification/clogging over time.
In this case, the shunt may need to be renewed with emergency intervention.
Signs of Shunt Infection and Complications
Since shunt systems are foreign bodies, it is possible for the body to react to this system or for microorganisms to settle in the system.
It is vital for parents to be vigilant for the following “red flag” signs:
- Fever and Vomiting: Unexplained high fever and gushing vomiting.
- Changes in Skin: Redness , swelling, or tenderness along the shunt line (neck or head area).
- Changes in Consciousness: Excessive sleepiness, difficulty waking up, or restlessness.
- Seizure: Onset of convulsions or seizures that did not exist before.
Assoc. Prof. Dr. Erdinç Özek; “A child with a shunt learns not to ‘live with a shunt’ throughout his life, but to be a healthy individual thanks to the shunt. However, the education of parents is as important as the success of the surgery. A family that realizes early that the shunt is broken or infected directly prevents permanent brain damage that may develop in the child. For us, surgery is just the beginning; The real success is in regular follow-up and strong communication with the family.”
Clinical Experience Note (Anonymous Case):
In a 7-year-old patient admitted to the emergency department due to shunt blockage, the existing constant pressure valve was removed and replaced with a ‘programmable gravity adjustable’ valve. Thanks to this technological change, the patient’s previous headaches caused by ‘overdrainage’ have completely disappeared. The patient was able to return to school 3 days after the operation and has now been having a trouble-free process for 2 years.
Frequently Asked Questions
Can a child with a shunt play sports?
Yes, children with shunts can participate in most sports activities. However, it is recommended to avoid heavy contact sports such as boxing and karate, which have a high risk of impact to the shunt system.
Does air travel affect shunt?
Under normal conditions, pressure changes during flight do not disrupt the shunt. However, patients with adjustable (magnet) valves should inform their doctors at safety passes and MRIs.
Should the shunt stay for life?
In most cases, yes. The shunt must remain until the brain’s absorption capacity returns. In some cases, the shunt is dysfunctional but the brain fluid finds its way (compensated hydrocephalus), the shunt is left in place but not intervened.
Resource and Expert Knowledge
This article has been prepared in light of Assoc. Prof. Dr. Erdinç Özek’s scientific studies on pediatric neurosurgery expertise, shunt technologies, and CSF dynamics, and current clinical protocols for 2026. Assoc. Prof. Dr. Erdinç Özek is a specialist who offers child-focused and technology-supported surgical solutions in the management of hydrocephalus.

